Europe PMC requires Javascript to function effectively.
Either your web browser doesn't support Javascript or it is currently turned off. In the latter case, please turn on Javascript support in your web browser and reload this page.

Search life-sciences literature (43,951,249 articles, preprints and more)
- Available from publisher site using DOI. A subscription may be required. Full text
- Citations & impact
- Similar Articles
A Plea for MERSQI: The Medical Education Research Study Quality Instrument.
Author information, affiliations.
Obstetrics and Gynecology , 01 Oct 2017 , 130(4): 686-690 https://doi.org/10.1097/aog.0000000000002091 PMID: 28885409
Abstract
Full text links .
Read article at publisher's site: https://doi.org/10.1097/aog.0000000000002091
References
Articles referenced by this article (10)
Association between funding and quality of published medical education research.
Reed DA , Cook DA , Beckman TJ , Levine RB , Kern DE , Wright SM
JAMA, (9):1002-1009 2007
MED: 17785645
Appraising the quality of medical education research methods: the Medical Education Research Study Quality Instrument and the Newcastle-Ottawa Scale-Education.
Cook DA , Reed DA
Acad Med, (8):1067-1076 2015
MED: 26107881
Predictive validity evidence for medical education research study quality instrument scores: quality of submissions to JGIM's Medical Education Special Issue.
Reed DA , Beckman TJ , Wright SM , Levine RB , Kern DE , Cook DA
J Gen Intern Med, (7):903-907 2008
MED: 18612715
An assessment of the methodologic quality of medical education research studies published in The American Journal of Surgery.
Reed DA , Beckman TJ , Wright SM
Am J Surg, (3):442-444 2009
MED: 19716888
Methodological rigor of quality improvement curricula for physician trainees: a systematic review and recommendations for change.
Windish DM , Reed DA , Boonyasai RT , Chakraborti C , Bass EB
Acad Med, (12):1677-1692 2009
MED: 19940573
Method and reporting quality in health professions education research: a systematic review.
Cook DA , Levinson AJ , Garside S
Med Educ, (3):227-238 2011
MED: 21299598
Update in internal medicine residency education: a review of the literature in 2010 and 2011.
Eaton JE , Reed DA , Aboff BM , Call SA , Chelminski PR , Thanarajasingam U , Post JA , Thomas KG , Dupras DM , Beckman TJ , West CP , Wittich CM , Halvorsen AJ , McDonald FS
J Grad Med Educ, (2):203-210 2013
MED: 24404261
Association Between Study Quality and Publication Rates of Medical Education Abstracts Presented at the Society of General Internal Medicine Annual Meeting.
Sawatsky AP , Beckman TJ , Edakkanambeth Varayil J , Mandrekar JN , Reed DA , Wang AT
J Gen Intern Med, (8):1172-1177 2015
MED: 25814265
Intrauterine Device Insertion During Cesarean Delivery: The Rising Tide of the Postdelivery Intrauterine Device.
Blumenthal PD , Goldthwaite LM
Obstet Gynecol, (1):1-2 2015
MED: 26241248
Screening, Prevention, and Treatment of Opioid Use Disorder During Pregnancy: Expectant Mothers Are Depending on You!
Obstet Gynecol, (1):1-3 2016
MED: 27275810
Citations & impact
Impact metrics, citations of article over time, alternative metrics.
")
Smart citations by scite.ai Smart citations by scite.ai include citation statements extracted from the full text of the citing article. The number of the statements may be higher than the number of citations provided by EuropePMC if one paper cites another multiple times or lower if scite has not yet processed some of the citing articles. Explore citation contexts and check if this article has been supported or disputed. https://scite.ai/reports/10.1097/aog.0000000000002091
Article citations, medical education research study quality instrument: an objective instrument susceptible to subjectivity..
Jaros S , Beck Dallaghan G
Med Educ Online , 29(1):2308359, 24 Jan 2024
Cited by: 0 articles | PMID: 38266115 | PMCID: PMC10810632
Self-directed learning assessment practices in undergraduate health professions education: a systematic review.
Taylor TAH , Kemp K , Mi M , Lerchenfeldt S
Med Educ Online , 28(1):2189553, 01 Dec 2023
Cited by: 2 articles | PMID: 36919556 | PMCID: PMC10026772
Publication rates of congress abstracts is associated with abstract quality: Evaluation of Turkish National Medical Education Congresses and Symposia between 2010 and 2014 using MERSQI.
Sarı E , Nteli Chatzioglou G , Aydın ÇY , Sarı F , Tokat T , Gürses İA
BMC Med Educ , 23(1):394, 30 May 2023
Cited by: 0 articles | PMID: 37254136 | PMCID: PMC10230785
A Modified Medical Education Research Study Quality Instrument (MMERSQI) developed by Delphi consensus.
Al Asmri M , Haque MS , Parle J
BMC Med Educ , 23(1):63, 25 Jan 2023
Cited by: 4 articles | PMID: 36698117 | PMCID: PMC9878889
Effectiveness of 3D-printed models prepared from radiological data for anatomy education: A meta-analysis and trial sequential analysis of 22 randomized, controlled, crossover trials.
Asghar A , Naaz S , Patra A , Ravi KS , Khanal L
J Educ Health Promot , 11:353, 31 Oct 2022
Cited by: 3 articles | PMID: 36567994 | PMCID: PMC9768753
Similar Articles
To arrive at the top five similar articles we use a word-weighted algorithm to compare words from the Title and Abstract of each citation.
Conference presentation to publication: a retrospective study evaluating quality of abstracts and journal articles in medical education research.
Stephenson CR , Vaa BE , Wang AT , Schroeder DR , Beckman TJ , Reed DA , Sawatsky AP
BMC Med Educ , 17(1):193, 09 Nov 2017
Cited by: 6 articles | PMID: 29121891 | PMCID: PMC5680828
J Gen Intern Med , 30(8):1172-1177, 01 Aug 2015
Cited by: 24 articles | PMID: 25814265 | PMCID: PMC4510227
Free full text in Europe PMC
To the Point: Integrating Patient Safety Education Into the Obstetrics and Gynecology Undergraduate Curriculum.
Abbott JF , Pradhan A , Buery-Joyner S , Casey PM , Chuang A , Dugoff L , Dalrymple JL , Forstein DA , Hampton BS , Hueppchen NA , Kaczmarczyk JM , Katz NT , Nuthalapaty FS , Page-Ramsey S , Wolf A , Cullimore AJ , APGO Undergraduate Medical Education Committee
J Patient Saf , 16(1):e39-e45, 01 Mar 2020
Cited by: 2 articles | PMID: 27465297
To the Point: The expanding role of simulation in obstetrics and gynecology medical student education.
Everett EN , Forstein DA , Bliss S , Buery-Joyner SD , Craig LB , Graziano SC , Hampton BS , Hopkins L , McKenzie ML , Morgan H , Pradhan A , Page-Ramsey SM , Undergraduate Medical Education Committee , Association of Professors of Gynecology and Obstetrics , Crofton , MD
Am J Obstet Gynecol , 220(2):129-141, 25 Oct 2018
Cited by: 6 articles | PMID: 30696555
Europe PMC is part of the ELIXIR infrastructure
A Plea for MERSQI: The Medical Education Research Study Quality Instrument
Affiliation.
- 1 Charles E. Schmidt College of Medicine, Florida Atlantic University, Boca Raton, Florida.
- PMID: 28885409
- DOI: 10.1097/AOG.0000000000002091
Objective: To describe the quality of educational scholarship presented at a large national conference of obstetrics and gynecology educators.
Methods: We reviewed Council on Resident Education in Obstetrics and Gynecology-Association of Professors of Gynecology and Obstetrics annual meeting abstracts from 2015 and 2016, published as supplements to Obstetrics & Gynecology. For this uncontrolled observational study, abstracts were reviewed and scored using the Medical Education Research Study Quality Instrument (MERSQI). Comparisons between types of submissions (oral presentations or posters), origin of the report (academic or community), setting (undergraduate, graduate, postgraduate), and focus of the study (tool development or evaluation) were made. Abstracts from award-winning presentations and full manuscripts were compared with the remaining abstracts. One- and two-tailed Student t tests with a two-sample unequal variance (heteroscedastic) test were performed with a significance threshold of P≤.05.
Results: One hundred eighty-six abstracts and articles were available, with 101 posters and 77 oral presentations that could be scored in all six of the MERSQI domains. The average MERSQI score was 9.05 (±1.90) with scores ranging from 5 to 13.5 (median 9). Abstracts from full-text articles scored more than 1 point higher than other abstracts (10.2 compared with 9.0, P<.001, Cohen's d=0.72). Statistically significant smaller magnitude differences were found comparing tool development with evaluation, academic with community studies, and for award with nonaward winners. No differences were found comparing oral and poster presentations.
Conclusion: The quality of educational scholarship presented at a national meeting of obstetrics and gynecology educators falls within the published range for other specialties. The MERSQI scoring system is a useful method for tracking and benchmarking the quality of medical education scholarship in obstetrics and gynecology.
Publication types
- Observational Study
- Biomedical Research / standards*
- Education, Medical / standards*
- Educational Measurement / methods
- Gynecology / education*
- Obstetrics / education*
- Research Report / standards*
")
An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- J Grad Med Educ
- v.11(1); 2019 Feb
Flipping the Classroom in Graduate Medical Education: A Systematic Review
Associated data.
Flipped classroom (FC) instruction has become increasingly common in graduate medical education (GME).
The purpose of this study was to profile the use of FC in the GME setting and assess the current status of research quality.
We conducted a systematic literature search of major health and social science databases from July 2017 to July 2018. Articles were screened to ensure they described use of the FC method in an Accreditation Council for Graduate Medical Education–accredited residency program and included research outcomes. Resulting articles were analyzed, described, and evaluated for research quality using the Kirkpatrick framework and the Medical Education Research Study Quality Instrument (MERSQI).
Twenty-two articles were identified, all of which were recently published. Five were only indirectly related to FC methods. Most studies reported Kirkpatrick-level outcomes. Studies involving resident learner opinions were generally positive. Pre-posttest studies resulted in large positive improvements in knowledge or skills attainment. Control group study results ranged from large positive (1.56) to negative effects (–0.51). Average MERSQI scores of 12.1 (range, 8.5–15.5) were comparable to GME research norms.
Conclusions
Varying methods for implementing and studying the FC in GME has led to variable results. While residents expressed a positive attitude toward FC learning, shortcomings were reported. Approximately half of the studies comparing the flipped to the traditional classroom reported better achievement under the FC design. As indicated by the MERSQI score, studies captured by this review, on average, were as rigorous as typical research on residency education.
Introduction
Medical education has been shifting from traditional, lecture-based teaching to approaches that promote higher-order thinking and active learning. 1 One particular approach, the flipped classroom (FC), has become increasingly popular in higher education, including medical education. 2 In this educational pedagogy, foundational content materials are studied by the learner independently through preclassroom activities, such as reading an article or textbook chapter, watching a multimedia presentation, or listening to a lecture in advance of classroom time. The classroom is reserved for applying foundational content knowledge in small group discussions involving clinical cases or more generic problem-solving. Conversely, in the traditional classroom, foundational content material is transmitted to learners through lectures that require review and reinforcement through study after class. 3 , 4
Advances in technology and the search for more effective approaches to teaching seem to be driving the shift to FC. 5 Active, self-directed learning—a necessary component of the FC learning model—is consistent with the needs of resident learners. 4 Additionally, this model is consistent with social, behavioral, and constructivist learning theories. 6 , 7 Group collaboration encourages modeling, scaffolding, and feedback that engage learners and facilitate the integration of new knowledge with old knowledge. 8 Compared to the traditional lecture, the FC promotes higher levels of cognitive processing as defined by Bloom's taxonomy. 8 – 10 As a result, increasing numbers of educators have adopted the FC across a variety of educational settings. 11 – 19
Literature on the FC has proliferated rapidly across health sciences education since its inception in 2007. 20 Numerous articles originated from pharmacy, nursing, or veterinary medicine education programs. 3 , 7 , 12 , 21 – 29 Both a recent systematic review and a meta-analysis covering the FC in medical education yielded very few articles on graduate medical education (GME). 3 , 30
The GME setting is more challenging than the undergraduate medical education (UME) setting. Resident learners may be less motivated by grades and more motivated by learning that facilitates patient care. Additionally, the GME learner's primary role is care provider while the UME learner's primary role is student. Given the marked differences in learning environments between UME and GME, and the FC's increasing popularity with residency programs, 19 a review specific to the effectiveness of the FC method in GME was needed. The goal of this systematic review is to profile the use of and assess the quality of the research literature on FC methods used in GME.
This study conforms to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for systematic reviews and was performed in accordance with best practice guidelines. 31
A health sciences librarian (S.J.S.) performed comprehensive searches of multiple databases, including PubMed, CINAHL Plus, Embase, Web of Science Core Collection, and ERIC, on July 27, 2017. Search alerts were used to gather new records through July 27, 2018. Major search terms and strategies are provided as online supplemental material. To identify additional manuscripts, we also searched MedEdPORTAL and reviewed bibliographies of included studies.
Inclusion and Exclusion Criteria
All articles published through July 2018 involving the use of FC in Accreditation Council for Graduate Medical Education (ACGME)–accredited residency programs were screened. We included articles that pertained to residents in any year of training from any medical specialty. Other inclusion criteria involved peer-reviewed, full-text articles that described some form of research or evaluation. We excluded articles that involved FC in non–medical education settings and at other levels of medical education, including UME, continuing medical education, or fellowship. We also excluded published abstracts. We did include articles that involved research or evaluation about preclassroom learning activities associated with FC. These activities are designed to introduce new knowledge to prepare learners for the classroom session, where they will apply the new knowledge from presession activities.
Two authors (A.M.K. and M.G.) independently screened titles and abstracts of retrieved articles, and subsequently selected articles for full-text review. Discrepancies were resolved by a third reviewer (J.M.). Two authors (J.M. and T.D.) independently reviewed the full-text articles and made the determination for inclusion in the final quality review. A third author (D.P.W.) adjudicated discrepancies at this stage.
Data Extraction
We extracted the following variables for each study: authors, publication year, medical specialty, level of trainees, education topic, FC method, specific intervention, number of FC participants, study design, and study outcomes. Research design terms used for classifying study design were derived from Campbell and Stanley. 32 Originally, 2 authors (J.M. and T.D.) independently performed data extraction using a worksheet to guide the process. Differences were adjudicated by a third reviewer (M.G.). Data from articles added later in the process were extracted by 2 other authors (A.M.K. and D.P.W.).
Quality Assessment
We used the modified Kirkpatrick framework to classify study outcomes of educational interventions according to impact level. 33 The modified Kirkpatrick classification levels are 1, measures of learner perceptions; 2a, self-reported changes in learner opinions; 2b, changes in knowledge or skills; 3, changes in learner behavior; 4a, change in professional practice; and 4b, change in patient's condition. When not provided, we also attempted to extract information needed to calculate associated Cohen's d effect sizes for each outcome. 34 , 35
Finally, we used the Medical Education Research Study Quality Instrument (MERSQI) to assess the quality of selected studies. 36 , 37 This 10-item scale provides a measure of methodological quality across 6 domains: study design, sampling, type of data, validity evidence, data analysis, and outcomes. Total MERSQI scores range from 2 (low-quality research) to 18 (high-quality research). Two authors (A.M.K. and J.M.) independently scored each article. An educational researcher (D.P.W.) adjudicated discrepancies in MERSQI scoring and Kirkpatrick level assignment.
Search Strategy
The Figure illustrates the systematic review process. The initial search yielded 2562 articles. After removing duplicates, 2123 studies were screened using titles and abstracts. Articles were excluded based on criteria outlined earlier, which resulted in 116 articles for full-text review. Of these 116, an additional 94 were excluded because they did not meet criteria. The final list of articles that met criteria for quality review included 22 articles. 8 , 38 – 58

PRISMA Diagram Illustrating Selection and Review Process of Articles Related to Flipped Classroom in Graduate Medical Education
Education Content
The 22 studies included in the final analysis are presented in Tables 1 and and2. 2 . All were published in the past 5 years (2014–2018), most (86%) in the past 3 years. Across all studies, approximately 985 learners were involved with a flipped classroom intervention. Thirteen medical specialties were represented, including anesthesiology, 46 , 49 , 50 , 57 emergency medicine, 8 , 38 , 44 , 52 , 58 internal medicine, 39 internal medicine–pediatrics, 43 neurology, 47 neurological surgery, 41 obstetrics and gynecology, 55 , 56 pathology, 42 pediatrics, 40 , 43 , 51 psychiatry, 45 radiology, 53 thoracic surgery, 48 and surgical intensive care. 54 All study designs were quantitative; however, a few gathered feedback through open-ended survey items.
Flipped Classroom (FC) Methodology in Graduate Medical Education
Abbreviations: PGY, postgraduate year; MK, medical knowledge; TBL, team-based learning; ACLS, advanced cardiovascular life support; PEM, pediatric emergency medicine; SICU, surgical intensive care unit; EEG, electroencephalogram.
Note: Dark shading indicates studies that focus predominantly on pre-class methods rather than the FC method.
Summary of Study Outcomes and Analysis
Abbreviations: MERSQI, Medical Education Research Study Quality Instrument; NA, not available; FC, flipped classroom; QIKAT, Quality Improvement Knowledge Application Tool; TBL, team-based learning; NR, not reported; QI, quality improvement; ADHD, Attention-Deficit/Hyperactivity Disorder.
Note: Dark shading indicates studies that focus predominantly on preclass methods rather than the FC method.
Authors of reviewed studies offered numerous reasons for incorporating the FC into their residency programs. Some suggested that using the FC was a solution to scheduling issues—either saving time in already saturated didactic schedules or providing schedule flexibility. 38 , 39 , 41 , 48 , 52 , 53 , 56 Others suggested that the FC method was selected to improve didactic instruction, motivate or engage learners, promote active learning, or prepare for more advanced levels of content material. 38 – 42 , 44 , 46 , 47 , 49 , 54
Residency programs adopted the FC method in 1 of 3 ways. Most commonly, authors described “occasional” use of the FC for a single lesson, usually to emphasize an important topic such as quality improvement, 39 , 43 resident-as-teacher skills, 40 using clinical guidelines, 51 echocardiography or electro-encephalograph interpretation, 47 , 54 , 57 or pediatric advanced life-support. 52 Other programs have replaced their entire didactic curriculum with FC sessions. 41 , 44 , 48 , 50 , 55 Three articles describe the use of FC for portions of their didactic curriculum: intern orientation, 38 , 49 , 53 reinforcement of important basic science principles, 42 , 45 , 46 and weekly didactics during 1- or 2-month rotations. 39 , 47 , 54 , 55 As proof-of-concept projects, Haspel and Lockhart designed FC instruction for delivery at national conferences. 42 , 45
Concerns about the FC surfaced in some of the literature, particularly around learner compliance with self-directed learning. Rose and colleagues discovered that residents did not accurately report time spent viewing video lectures in preparation for FC activities. 52 Residents in the Young et al study suggested that time for preclass preparation was a weakness of the FC format. 58 Without adequate preclass preparation, learners are unable to effectively participate in applying content knowledge during the in-class meeting. Consequently, several studies involved the production of innovative methods for delivering preclass content such as podcast lectures, interactive electronic modules, or multimedia textbooks. These materials were designed specifically to persuade learners into completing the self-directed learning required for constructive participation during in-class activities. 41 , 45 , 47 , 49 , 50 , 52 , 57
Study Outcomes
Five of the selected articles focused more on preclass methods and less about the FC method itself. Lockhart and colleagues assessed the implementation of a small, private, online course. 45 Moeller et al and Vasilopoulos et al studied the effectiveness of podcast lectures. 47 , 57 Rose and colleagues studied the impact of embedding multiple-choice questions into instructional videos, 52 and Ortega et al evaluated a multimedia, interactive textbook. 50 Since none of these studies reported outcomes related to both preclass and in-class FC methods, they were not subject to Kirkpatrick classification.
Level 1 Outcomes–Perception:
Most of the 7 studies that evaluated Kirkpatrick Level 1 outcomes were not designed for control group comparisons or change over time. 41 – 44 , 48 , 51 , 58 Accordingly, effect sizes were not appropriate for Level 1 articles. An exception was the article by King and colleagues that compared ratings of curriculum components before and after the program switched from lecture-based to FC methods. 44 Residents rated all components higher under the FC model, but only 2 (adult and pediatric case conferences) were deemed significantly higher in quality and value, which yielded large effect sizes (d = 1.19 and 1.10, respectively). 44
Level 2a Outcomes–Change in Opinion:
Almost a third of the articles reported changes in learner opinions about the FC, the content taught, or the learners themselves. 38 – 40 , 43 , 46 , 49 , 53 , 54 Changes in opinion about the FC method were observed in a control group study and a pre-post study, both yielding large effect sizes of 1.1 and 0.95, respectively. 39 , 46 Residents improved their opinions about teaching in a pre-post study of resident-as-teacher skills, which also yielded a large effect (0.95). 40 Studies that reported changes in self-efficacy, confidence, comfort, or anxiety yielded smaller effect sizes, ranging from 0.32–0.84. 39 , 49 An exception was the Bonnes resident-as-teacher study, which generated a large 1.68 effect size for change in self-assessment of resident teaching skills. 39 Effect sizes could not be calculated for the remaining articles reporting Level 2a outcomes. 38 , 43 , 53 , 54
Level 2b Outcomes–Change in Knowledge or Skills:
A third of the articles reported changes in knowledge or skills that came from controlled studies involving either parallel or historic control groups. 8 , 39 , 41 , 44 , 46 , 51 , 55 , 56 Effect sizes for these studies ranged from large (1.56) to negative (–0.51). An additional 5 articles reported changes in knowledge or skills that came from pre-posttest studies, 2 of which had associated effect size that were either large (0.81) 40 or very large (2.73). 38 Effect sizes could not be calculated for the other 3 articles. 43 , 53 , 54
Level 3 Outcomes–Change in Behaviors:
Only 2 studies reported changes in behaviors: one involving increases in self-directed learning outside of class, 44 and the other reporting inflated, self-reported, preclass preparation times when compared to actual preparation times. 52 The effect size for the first was large (0.85), 44 but the effect size for the second could not be calculated. 52
Study Quality
Cook and Reed provided a table of normative data for interpreting MERSQI scores. 36 A mean score of 10 (range, 5–16) was generated through a review of 210 articles covering medical education. 36 For the specific topic of residency education, the mean MERSQI of 12.9 (range, 9–15.6) was generated through a review of 97 articles. This is considerably higher than the mean MERSQI score of 10.9 we observed for the 22 articles reviewed (range, 4–15.5, SD = 3.08). By dropping 4 pilot or proof-of-concept studies, which had only Level 1 outcomes from our analysis, 45 , 47 , 50 , 58 the average MERSQI score would be more comparable to the normative data reported by Cook and Reed (M = 12.1; range, 8.5–15.5; SD = 1.93). 36
Looking at individual MERSQI items suggests that research on the FC in GME is still in its infancy. The literature review included numerous articles that were considered pilot or proof-of-concept studies. Some specifically targeted investigations into developing content delivery methods for preclass preparation such as video lectures, 43 , 46 podcasts, 41 , 51 or a multimedia interactive textbook. 44 Only half of the articles reviewed used experimental or quasi-experimental designs with control groups (either a control arm or historical controls). 8 , 39 , 41 , 44 , 46 , 48 , 49 , 51 , 55 , 56 The other half were pre-experimental, involving only 1 group pre-posttest or posttest-only designs. 38 , 40 , 42 , 43 , 45 , 47 , 49 , 52 – 54 , 57 , 58 Only 5 studies involved cross-institutional collaborations. 8 , 36 , 39 , 46 , 47 While almost three-quarters used objective measures, very few articles provided validity evidence in the form of construct or content validity. Furthermore, articles investigating the relationship between relevant variables were limited. However, more than three-quarters (77%, 17 of 22) of the studies used appropriate analyses and almost 70% (15 of 22) implemented inferential statistics to analyze outcome variables such as knowledge or skills.
This systematic review of FC application in GME yielded several important findings. While still in its early stages, research on the FC in GME has increased substantially over the past 5 years, with 17 of 22 articles being published since 2016. We discovered use of the FC in at least 13 types of residency programs, suggesting that the teaching method can be broadly adopted across a variety of GME settings. Reasons for using the FC and specific techniques on how it was applied vary greatly across programs, suggesting that it is not a one-method-fits-all intervention. We found that the FC has been applied to entire residency programs or, on a more limited scale, within rotations or to cover specific topics. The method has also been used across institutions to prepare learners for specialized topics, or to capitalize on educator expertise.
We attribute the rise of interest in the FC in GME to medical educators' desire to find better teaching methods, recognizing that this method is suitable for residents and can be adapted to the GME setting. The self-directed learning component gives residents more control, allowing them to learn content at their own pace and during times outside of their clinical responsibilities. Consistent with social learning theory, the FC provides a venue for collaborative learning where learners publicly demonstrate their application of knowledge during small group discussion of patient cases and problems. 7 , 8 Learner enthusiasm for the FC method and documented improvements in knowledge and skills make the FC an attractive alternative to the traditional lecture-based education model.
Medical educators have suggested that their interest in the FC is associated with making more effective use of instructional time, providing more structure for self-directed learning outside of class, or motivating residents to spend more time outside of clinical responsibilities engaged in study. The FC requires learners to complete self-directed learning activities to participate during in-class sessions. This was a concern among graduate medical educators because residents have clinical responsibilities that compete for their time. We believe many studies created more interesting methods for delivering preclassroom content because of this concern.
F. Chen and colleagues' earlier systematic review of the FC approach in medical education found that the “majority of literature has been carried out in UME.” 3 Additionally, their review suggested that research up to that point “lacked strong evidence for the effectiveness of FCs.” 3 A subsequent comprehensive meta-analysis by K.S. Chen et al covered a relatively small number of studies involving medical education and only one that involved residency education. 30 This group of authors tentatively suggested an advantage of the FC over lecture-based methods; however, they expressed concern about this interpretation due to extreme diversity in methods. Our systematic review focused solely on the use of the FC in ACGME-accredited residency programs. Like K.S. Chen, we confronted diversity in research methods, but also diversity in how the FC was applied and the content covered. In contrast with F. Chen, and comparable to K.S. Chen, we found that learners generally find the FC approach acceptable and evidence supports that the FC is as good as a traditional didactic approach (introducing topics through lecture or during a face-to-face meeting followed by readings and study of educational materials).
This systematic review of the FC literature has some limitations. While we employed what we think is a comprehensive search strategy with the help of an experienced medical librarian, it is possible that we did not include more esoteric terms that refer to methods associated with FCs. For example, we did not use the term “problem-based learning,” which is a method that typically describes a comprehensive approach to education, but could be associated with the FC format on a more limited basis. In addition, we made the decision to exclude non-ACGME residency programs and US fellowship programs. This decision was based on the variability of education structures found outside the United States and variability in size and purpose of fellowships. These decisions may have restricted the generalizability of our findings.
The assessment of higher-level outcomes, such as changes in learner behaviors or patient outcomes, remains a challenge in medical education. 36 These outcomes are difficult to assess because they rarely can be attributed to a single educational intervention. Despite these challenges, we were heartened to find an increasing number of studies that generated Kirkpatrick levels 2a, 2b, and 3 outcomes, many studies that employed objective measures, and an increasing number of studies that employed more rigorous research designs. Future research on the FC in GME should focus on higher-level outcomes such as changes in behaviors, clinical practice, and patient outcomes. 33
The FC pedagogical approach in GME has been implemented in a variety of ways and studied with a variety of methods, which has yielded variable results. Using MERSQI scores, studies evaluating the efficacy of the FC were somewhat less rigorous than typical medical education research studies; however, if pilot and proof-of-concept studies are eliminated, the average MERSQI score was comparable to that of other medical education research studies. The studies that evaluated resident satisfaction or efficacy concluded that residents held generally positive opinions about the FC. For studies that evaluated learning outcomes, the results were mixed: slightly more than half of the studies using a control group for comparison found positive learning results. Future studies of FC in GME should include higher-level outcomes (changes in knowledge, behaviors, or patient outcomes) and assessment of preclassroom assignment completion.
Supplementary Material
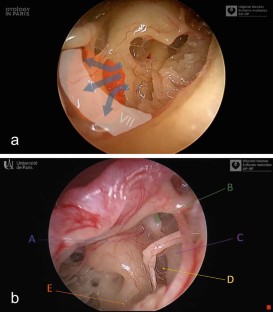
Educational endoscopic videos improve teaching of middle ear anatomy
- Published: 20 April 2024
Cite this article
- Valentino Caputo ORCID: orcid.org/0009-0006-3635-6035 1 ,
- Françoise Denoyelle ORCID: orcid.org/0000-0003-4338-9258 1 &
- François Simon ORCID: orcid.org/0000-0003-0082-538X 1
Explore all metrics
Videos and images are becoming an educational tool in every domain. The objective was to assess the contribution of short educational endoscopic videos in learning the complex anatomy of the tympanic cavity.
We conducted a prospective study amongst all the otolaryngology residents in 2021 in the greater Paris area ( n = 74), from the first year to fifth year. We divided the residents into two groups who had the same 30-min anatomy class based on anatomical drawings. The second group had a 4-min endoscopic educational video at the end, whereas the first group did not. A video test of 10 surgical situations with each time 5 anatomic structures to identify was created. All the residents took the test just after the class, and 1 month later to assess long-term memory. The MERSQI score (design to assess the quality of educational studies) applied to our study was calculated.
The two groups were comparable in terms of training. The “video” group had significantly better results in the first test, mean score 24.40/50 (± 11.7) versus 16.74/50 (± 11.1) (p = 0.005) and also at 1 month, mean score 23.25/50 (± 12.3) versus 18.01/50 (± 11.3) (p = 0.035). The score in each group, and the difference between both groups, increased with resident seniority. The MERSQI score of our study was 14.5/18.
This study highlights the educational value of videos to help memorise complex 3D anatomy such as in the tympanic cavity.
This is a preview of subscription content, log in via an institution to check access.
Access this article
Price includes VAT (Russian Federation)
Instant access to the full article PDF.
Rent this article via DeepDyve
Institutional subscriptions
Data availability
Not applicable.
Isaacson G (2014) Endoscopic anatomy of the pediatric middle ear. Otolaryngol Head Neck Surg 150(1):6–15
Article PubMed Google Scholar
Marchioni D, Molteni G, Presutti L (2011) Endoscopic anatomy of the middle ear. Indian J Otolaryngol Head Neck Surg. 63(2):101–113
Article PubMed PubMed Central Google Scholar
Anschuetz L, Alicandri-Ciufelli M, Wimmer W, Bonali M, Caversaccio M, Presutti L (2019) The endoscopic anatomy of the cochlear hook region and fustis: surgical implications. Acta Otorhinolaryngol Ital 39(5):353–357
Article CAS PubMed PubMed Central Google Scholar
Li B, Doan P, Gruhl RR, Rubini A, Marchioni D, Fina M (2018) Endoscopic anatomy of the tensor fold and anterior attic. Otolaryngol Head Neck Surg 158(2):358–363
Anschuetz L, Presutti L, Marchioni D, Bonali M, Wimmer W, Villari D et al (2018) Discovering middle ear anatomy by transcanal endoscopic ear surgery: a dissection manual. J Vis Exp. https://doi.org/10.3791/56390
Soloperto D, Ronzani G, Sacchetto L, Marchioni D (2023) Endoscopic findings on facial nerve anatomy during exclusive endoscopic stapedotomy: clinical considerations and impact on surgical results. J Int Adv Otol. 19(6):503–510
Poe DS (1992) Transtympanic endoscopy of the middle ear. Oper Tech Otolaryngol Head Neck Surg 3(4):239–244
Article Google Scholar
Poon C, Stevens SM, Golub JS, Pensak ML, Samy RN (2017) Pilot study evaluating the impact of otology surgery videos on otolaryngology resident education. Otol Neurotol 38(3):423–428
Chan LK, Patil NG, Chen JY, Lam JCM, Lau CS, Ip MSM (2010) Advantages of video trigger in problem-based learning. Med Teach 32(9):760–765
Jang HW, Kim KJ (2014) Use of online clinical videos for clinical skills training for medical students: benefits and challenges. BMC Med Educ déc 14(1):56
Grüter AAJ, Toorenvliet BR, Belgers EHJ, Belt EJT, Van Duijvendijk P, Hoff C et al (2023) Nationwide standardization of minimally invasive right hemicolectomy for colon cancer and development and validation of a video-based competency assessment tool (the Right study). Br J Surg. https://doi.org/10.1093/bjs/znad404
Article PubMed Central Google Scholar
Anschuetz L, Huwendiek S, Stricker D, Yacoub A, Wimmer W, Caversaccio M (2019) Assessment of middle ear anatomy teaching methodologies using microscopy versus endoscopy: a randomized comparative study. Anat Sci Educ sept 12(5):507–517
Anschuetz L, Siggemann T, Dür C, Dreifuss C, Caversaccio M, Huwendiek S (2020) Teaching middle ear anatomy and basic ear surgery skills: a qualitative study comparing endoscopic and microscopic techniques. Otolaryngol Head Neck Surg. https://doi.org/10.1177/0194599820977191
Bennett ML, Zhang D, Labadie RF, Noble JH (2016) Comparison of middle ear visualization with endoscopy and microscopy. Otol Neurotol 37(4):362–366
Bowdler DA, Walsh RM (1995) Comparison of the otoendoscopic and microscopic anatomy of the middle ear cleft in canal wall-up and canal wall-down temporal bone dissections. Clin Otolaryngol 20(5):418–422
Article CAS PubMed Google Scholar
Darras KE, de Bruin ABH, Nicolaou S, Dahlström N, Persson A, van Merriënboer J et al (2018) Is there a superior simulator for human anatomy education? How virtual dissection can overcome the anatomic and pedagogic limitations of cadaveric dissection. Med Teach 40(7):752–753
Simon F, Peer S, Michel J, Bruce IA, Cherkes M, Denoyelle F et al (2021) Guidelines (instructional videos in otorhinolaryngology by: a consensus on surgical videos in ear, nose, and throat). Laryngoscope. https://doi.org/10.1002/lary.29020
Reed DA, Cook DA, Beckman TJ, Levine RB, Kern DE, Wright SM (2007) Association between funding and quality of published medical education research. JAMA 298(9):1002
Reed DA, Beckman TJ, Wright SM, Levine RB, Kern DE, Cook DA (2008) Predictive validity evidence for medical education research study quality instrument scores: quality of submissions to jgim’s medical education special issue. J Gen Intern Med. 23(7):903–7
Chauvet P, Botchorishvili R, Curinier S, Gremeau AS, Campagne-Loiseau S, Houlle C et al (2020) What is a good teaching video? Results of an online international survey. J Minim Invasive Gynecol 27(3):738–747
Green JL, Suresh V, Bittar P, Ledbetter L, Mithani SK, Allori A (2019) The utilization of video technology in surgical education: a systematic review. J Surg Res 235:171–180
Crawshaw BP, Steele SR, Lee EC, Delaney CP, Mustain WC, Russ AJ et al (2016) Failing to prepare is preparing to fail: a single-blinded, randomized controlled trial to determine the impact of a preoperative instructional video on the ability of residents to perform laparoscopic right colectomy. Dis Colon Rectum. 59(1):28–34
Farquharson AL, Cresswell AC, Beard JD, Chan P (2013) Randomized trial of the effect of video feedback on the acquisition of surgical skills. Br J Surg. 100(11):1448–53
Ahmet A, Gamze K, Rustem M, Sezen KA (2018) Is video-based education an effective method in surgical education? A systematic review. J Surg Educ 75(5):1150–1158
Lyon DR, Colletta MD, Biggs P, Pierce DC, Tarima SS, Visotcky A et al (2022) Can we learn faster? A pilot study using surgical videos to improve pediatric tonsillectomy competency in OSATS. Int J Pediatr Otorhinolaryngol 163:111366
Download references
Author information
Authors and affiliations.
Hospital Necker Enfants Malades, Paris, France
Valentino Caputo, Françoise Denoyelle & François Simon
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Valentino Caputo .
Additional information
Publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Reprints and permissions
About this article
Caputo, V., Denoyelle, F. & Simon, F. Educational endoscopic videos improve teaching of middle ear anatomy. Eur Arch Otorhinolaryngol (2024). https://doi.org/10.1007/s00405-024-08658-1
Download citation
Received : 18 February 2024
Accepted : 03 April 2024
Published : 20 April 2024
DOI : https://doi.org/10.1007/s00405-024-08658-1
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Educational
- Find a journal
- Publish with us
- Track your research
COMMENTS
The Medical Education Research Study Quality Instrument (MERSQI) is widely used to appraise the methodological quality of medical education studies. However, the MERSQI lacks some criteria which could facilitate better quality assessment. The objective of this study is to achieve consensus among experts on: (1) the MERSQI scoring system and the relative importance of each domain (2 ...
The Medical Education Research Study Quality Instrument (MERSQI) was introduced in 2007 to appraise the methodological quality of studies of medical education . MERSQI evaluates the quality of the research itself rather than the quality of the reporting and the authors [ 1 ] excluded elements such as "importance of research questions" and ...
Purpose: The Medical Education Research Study Quality Instrument (MERSQI) and the Newcastle-Ottawa Scale-Education (NOS-E) were developed to appraise methodological quality in medical education research. The study objective was to evaluate the interrater reliability, normative scores, and between-instrument correlation for these two instruments.
However, given that the MERSQI has been used as a means of determining the quality of medical education research [Citation 3, Citation 4], using the MERSQI to rate highly cited medical education research has uncovered some flaws with the instrument with regard to specific items. If an overall score continues to be used for screening purposes ...
Background: The Medical Education Research Study Quality Instrument (MERSQI) is widely used to appraise the methodological quality of medical education studies. However, the MERSQI lacks some criteria which could facilitate better quality assessment. The objective of this study is to achieve consensus among experts on: (1) the MERSQI scoring system and the relative importance of each domain (2 ...
The authors present a modification of a commonly used study quality instrument, the Medical Education Research Study Quality Instrument (MERSQI), using a modified Delphi technique to reach consensus among experts in the field of medical education, with the aim of identifying any changes required in the scoring system and relative importance of ...
A Modied Medical Education Research Study Quality Instrument (MMERSQI) developed by Delphi consensus Mansour Al Asmri1, M. Sayeed Haque2 and Jim Parle3* Abstract Background The Medical Education Research Study Quality Instrument (MERSQI) is widely used to appraise the methodological quality of medical education studies. However, the MERSQI ...
The Medical Education Research Study Quality Instrument (MERSQI) was introduced in 2007 1 and has gained acceptance alongside other checklist tools for the evaluation of, and planning for, various other types of research or reviews. Although the MERSQI is not the only evaluation tool for educational research, it has gained wider adoption than the alternate Newcastle-Ottawa scale. 2 The MERSQI ...
Keywords Methodological quality, Quantitative studies, Delphi, Medical education, Quality instrument Background e Medical Education Research Study Quality Instru - ment (MERSQI) was introduced in ...
Secondly, the quality of presented abstracts was assessed with the Medical Education Research Study Quality Instrument (MERSQI) scale. Overall publication rate for the abstracts was 11.3%.
Background: The medical education research study quality instrument (MERSQI) was designed to appraise medical education research quality based on study design criteria. As with many such tools, application of the results may have unintended consequences. This study applied the MERSQI to published medical education research identified in a bibliometric analysis.
However, two instruments have been developed and used in recent years to appraise the methodological quality of studies of medical education—namely, the Medical Education Research Study Quality Instrument (MERSQI) 8 and the Newcastle-Ottawa Scale-Education (NOS-E). 9 A description and detailed validation of the MERSQI were published with ...
However, given that the MERSQI has been used as a means of determining the quality of medical education research [3,4], using the MERSQI to rate highly cited medical education research has uncovered some flaws with the instrument with regard to specific items. If an overall score continues to be used for screening purposes, revisions should be ...
The quality of included studies was assessed using the Medical Education Research Study Quality Instrument (MERSQI) [7]. Evidence was tabulated and further described by narrative review, according ...
For this uncontrolled observational study, abstracts were reviewed and scored using the Medical Education Research Study Quality Instrument (MERSQI). Comparisons between types of submissions (oral presentations or posters), origin of the report (academic or community), setting (undergraduate, graduate, postgraduate), and focus of the study ...
The MERSQI is a ten-item instrument designed to assess the methodological quality of experimental, quasi-experimental, and observational medical education research studies.10 The ten items reflect six domains of study quality: study design, sampling, data type (subjective or objective), validity of assessments, data analysis, and outcomes. The ...
For this uncontrolled observational study, abstracts were reviewed and scored using the Medical Education Research Study Quality Instrument (MERSQI). Comparisons between types of submissions (oral presentations or posters), origin of the report (academic or community), setting (undergraduate, graduate, postgraduate), and focus of the study ...
The MMERSQI, in building on the success of the MERSQI, may help further establish a reference standard of quality measures for many medical education studies and be a reference standard of quality measures for many medical education studies. Background The Medical Education Research Study Quality Instrument (MERSQI) is widely used to appraise the methodological quality of medical education ...
Finally, we used the Medical Education Research Study Quality Instrument (MERSQI) to assess the quality of selected studies. 36, 37 This 10-item scale provides a measure of methodological quality across 6 domains: study design, sampling, type of data, validity evidence, data analysis, and outcomes. Total MERSQI scores range from 2 (low-quality ...
The Medical Education Research Study Quality Instrument (MERSQI) has been used frequently to assess the methodological quality of medical education but not for dental education. The present study aimed to assess the methodological quality using MERSQI scores of articles published in the Journal of Dental Education (JDE) and the European Journal ...
MERSQI is a measurement score designed in 2007, validated and widely used to evaluate methodological quality of medical education research (24). It consists of ten items, re ecting six domains of ...
Finally, to assess the quality of our educational study, we used the Medical education research study quality instrument (MERSQI score) . This score is based on six domains: study design, sampling, type of data, validity of evaluation instrument, data analysis and outcomes.
Methodological quality of included studies was assessed using the modified medical education research study quality instrument (MERSQI) checklist. Heterogeneity in data reporting on types of tools, data collection, study design, definition of expertise (novice vs. experts) and statistical values prevented a meaningful meta-analysis.